



Recently, a five year old girl saw me with complaints of "my mouth hurts" and "my tummy hurts." Her mother noticed sores in her mouth several days ago. Her medical history was unremarkable, she was a healthy active young girl. Upon examination, she had a temperature of 100.6 and a couple of small sores in her mouth. Interestingly, she also had a rash on her hands. Reassurance was given to both the mother and the girl and she recovered nicely in several days.
Hand Foot and Mouth Disease is a viral illness that affects young children, typically under ten years of age. It is most commonly caused by coxsackieviruses (Enterovirus genus), members of the Picornaviridae family. HFMD is contagious and spread by nasal secretions, saliva, fecal material, and aerosolized droplets. Daycares have a high incidence of HFMD. It is more common during the summer and autumn months. Children are contagious one week prior to the onset of symptoms and potentially several weeks after resolution.
The signs and symptoms include (but not limited to):
1. Fever
2. Fatigue
3. Cough
4. Abdominal pain
5. Sore throat
6. Poor appetite
The rash and sores develop 12 to 36 hours later. The oral sores are painful, red, blister-like lesions located on the tongue, inner cheeks, or gums. The rash on the palms, soles of feet, or buttocks are not itchy, red, and possibly blistery. The rash and sores can last for five to seven days.
HFMD is not usually serious and self-limiting (will resolve with time). Rare complications include viral meningitis, myocarditis, and encephalitis.
Treatment includes:
1. Fluids
2. Supportive care
3. Tylenol or ibuprofen for the pain
4. Popsicles/ice cream for the oral pain
5. Warm salt water rinses without swallowing (1/2 teaspoon of salt with one cup of warm water)
6. Time...HFMD will usually resolve in 7-10 days
Prevention includes:
1. Good hygiene
2. Hand washing (twenty seconds)
3. Do not rupture blisters
4. Avoid close contact with patients diagnosed with HFMD
5. Keeping toys and surfaces clean
Call the doctor immediately if the child develops any of the following symptoms:
1. Fever higher than 100.4° Fahrenheit (38° Celsius) for infants younger than 6 months and higher than 102° Fahrenheit (38.8° Celsius) for older kids
2. Poor appetite or trouble feeding
3. Difficulty breathing
4. Convulsions
5. Unusual sleepiness
6. Severe headache, especially with vomiting, confusion, unusual sleepiness, or convulsions
7. Neck stiffness
Please note Hand Foot and Mouth Disease is not Foot (Hoof) and Mouth Disease.
Call your primary physician for more information. Hope this was informative!
Sunday, November 29, 2009
Friday, November 27, 2009
Osgood Schlatter Disease
A 13 year old female presented to the office with bilateral (both) knee pain. She stated the pain was worse when running but better on rest. The pain started during field hockey season and has persisted for months. She denied any trauma or injury. Exam was remarkable for tenderness right below both knee caps. Radiograph findings were consistent with Osgood Schlatter Disease.
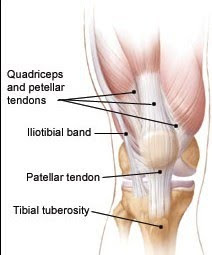
Osgood Schlatter disease is a benign condition that causes pain, tenderness, and/or swelling below the knee cap, over the shin bone (tibia). It is typically seen in active teenagers eleven to fifteen years of age (during the growth spurt years) with a male to female ratio of 3:1. The pain is caused by stress on the patellar tendon that attaches to the quadriceps at the front of the thigh to the tibial tuberosity. The repeated stress from running, jumping, gymnastics, dancing, etc, causes inflammation and possible avulsion fractures at the site which leads to the pain and a bony lump. The pain is typically worse during activity.
The signs and symptoms include:
1. Pain on the upper shin, below the knee cap...can be intense!
2. Swelling at the site
3. Tender bony lump
4. Tight quadriceps
Osgood-Schlatter disease affects about 20 percent of adolescents who participate in sports. The sports include soccer, football, basketball, ballet, gymnastics, volleyball, field hockey, lacrosse, etc...
Diagnosis is made by history, physical, and x-rays.
Treatment includes:
RICE
R = Rest the knee from the painful activity.
I = Ice the affected area for 20 minutes, 3 times a day.
C = Compress the painful area with an elastic bandage.
E = Elevate the leg.
Anti-inflammatories (Motrin, Advil) also will help with the pain.
Physical therapy is utilized to strengthen the quadriceps and hamstrings. Some examples include straight leg raises, quad contractions, and leg curls.
The pain may last for several weeks to several months. Physical activity may have to be restricted depending on the severity of the pain.
With adequate time, treatment, and rest, Osgood Schlatter disease should resolve. Rarely does OSD occur after the growth spurt years due to the strengthening of the patellar tendon.
For more information, contact your primary physician.
Osgood Schlatter disease is a benign condition that causes pain, tenderness, and/or swelling below the knee cap, over the shin bone (tibia). It is typically seen in active teenagers eleven to fifteen years of age (during the growth spurt years) with a male to female ratio of 3:1. The pain is caused by stress on the patellar tendon that attaches to the quadriceps at the front of the thigh to the tibial tuberosity. The repeated stress from running, jumping, gymnastics, dancing, etc, causes inflammation and possible avulsion fractures at the site which leads to the pain and a bony lump. The pain is typically worse during activity.

The signs and symptoms include:
1. Pain on the upper shin, below the knee cap...can be intense!
2. Swelling at the site
3. Tender bony lump
4. Tight quadriceps
Osgood-Schlatter disease affects about 20 percent of adolescents who participate in sports. The sports include soccer, football, basketball, ballet, gymnastics, volleyball, field hockey, lacrosse, etc...
Diagnosis is made by history, physical, and x-rays.
Treatment includes:
RICE
R = Rest the knee from the painful activity.
I = Ice the affected area for 20 minutes, 3 times a day.
C = Compress the painful area with an elastic bandage.
E = Elevate the leg.
Anti-inflammatories (Motrin, Advil) also will help with the pain.
Physical therapy is utilized to strengthen the quadriceps and hamstrings. Some examples include straight leg raises, quad contractions, and leg curls.
The pain may last for several weeks to several months. Physical activity may have to be restricted depending on the severity of the pain.
With adequate time, treatment, and rest, Osgood Schlatter disease should resolve. Rarely does OSD occur after the growth spurt years due to the strengthening of the patellar tendon.
For more information, contact your primary physician.
Sunday, November 22, 2009
Lyme Disease
A 15 year old female presented to the office with a month long complaint of fatigue and body aches. Otherwise she felt well. Her medical history was unremarkable. She denied pregnancy. Her exam was unremarkable with no evidence of rash. Laboratory investigation was performed including a blood count, thyroid, glucose, and Lyme antibody. Her Lyme test was positive and then confirmed by a Western Blot test. She was given 21 days of Doxycycline and recovered well.
Lyme disease is the most common tick borne illness in the United States. The disease was first reported in 1975 in Lyme, Connecticut due to a cluster of cases involving arthritis in children. Since then, there have been thousands of cases with an annual incidence of 0.5% in endemic areas. The peak months are from May to August and the high risk states include Connecticut, Delaware, Maryland, Rhode Island, New Jersey, New York, and Pennsylvania.
The causative bacteria is Borrelia burgdorferi (type of spirochete). The organism is carried by the white tail deer and the white footed mouse. The bacteria is transmitted from the animal to human by the deer tick (Ixodes). If the tick is removed within 24 hours, the chance of contracting the disease is virtually zero percent. Also, less than 5% of tick bites result in Lyme Disease.
deer and the white footed mouse. The bacteria is transmitted from the animal to human by the deer tick (Ixodes). If the tick is removed within 24 hours, the chance of contracting the disease is virtually zero percent. Also, less than 5% of tick bites result in Lyme Disease.
The signs and symptoms include:
1. "Flu-like" symptoms usually several days to several weeks following the tick bite
2. Erythema Migrans (characteristic rash of Lyme Disease)
3. Joint pain
4. Fever
5. Fatigue
6. Headache
7. Neck pain
Erythema Migrans is defined by the CDC as a skin lesion that typically begins as a r ed spot and expands over a period of days to weeks to form a large round lesion, at least 5 cm (about 2 inches) across. As it grows, it may look like a bull's eye rash.
ed spot and expands over a period of days to weeks to form a large round lesion, at least 5 cm (about 2 inches) across. As it grows, it may look like a bull's eye rash.
The symptoms, if untreated, can progress to severe arthritis, cardiac problems, neurologic complications, ocular problems, gastrointestinal complaints, and hepatitis.
Diagnosis is made by blood work (Lyme titer via ELISA and Western Blot). If there are neurologic symptoms, the CSF needs to be tested for meningitis.
Treatment includes:
1. Tick removal
2. Contact your primary physician
3. Antibiotics (Doxycycline, Amoxicillin, or Cefuroxime) for at least 21 days
4. If the symptoms are severe, IV antibiotics may be necessary
Prevention includes:
1. Wear enclosed shoes and light-colored clothing to spot ticks
2. Check clothes and any exposed skin frequently for ticks while outdoors
3. Stay on cleared, well-traveled trails
4. Use insect repellant containing DEET (Diethyl-meta-toluamide) on skin or clothes
5. Avoid sitting directly on the ground or on stone walls
6. Keep long hair tied back
7. Do a full-body tick-check at the end of the day (also check children and pets)
To remove a tick, follow these steps:
1. Using a pair of pointed tweezers, grasp the tick by the head right where it enters the skin. Do not grasp the tick by the body.
2. Pull firmly and steadily directly outward. Dn not twist the tick out or apply petroleum jelly, a hot match, alcohol or any other irritant to the tick in an attempt to get it to back out.
3. Place the tick in a vial of alcohol to kill it.
4. Clean the bite wound
Contact your primary physician for more information.
Also check the CDC link on Lyme Disease.
Have a safe Thanksgiving Holiday!
Lyme disease is the most common tick borne illness in the United States. The disease was first reported in 1975 in Lyme, Connecticut due to a cluster of cases involving arthritis in children. Since then, there have been thousands of cases with an annual incidence of 0.5% in endemic areas. The peak months are from May to August and the high risk states include Connecticut, Delaware, Maryland, Rhode Island, New Jersey, New York, and Pennsylvania.
The causative bacteria is Borrelia burgdorferi (type of spirochete). The organism is carried by the white tail
 deer and the white footed mouse. The bacteria is transmitted from the animal to human by the deer tick (Ixodes). If the tick is removed within 24 hours, the chance of contracting the disease is virtually zero percent. Also, less than 5% of tick bites result in Lyme Disease.
deer and the white footed mouse. The bacteria is transmitted from the animal to human by the deer tick (Ixodes). If the tick is removed within 24 hours, the chance of contracting the disease is virtually zero percent. Also, less than 5% of tick bites result in Lyme Disease.The signs and symptoms include:
1. "Flu-like" symptoms usually several days to several weeks following the tick bite
2. Erythema Migrans (characteristic rash of Lyme Disease)
3. Joint pain
4. Fever
5. Fatigue
6. Headache
7. Neck pain
Erythema Migrans is defined by the CDC as a skin lesion that typically begins as a r
 ed spot and expands over a period of days to weeks to form a large round lesion, at least 5 cm (about 2 inches) across. As it grows, it may look like a bull's eye rash.
ed spot and expands over a period of days to weeks to form a large round lesion, at least 5 cm (about 2 inches) across. As it grows, it may look like a bull's eye rash.The symptoms, if untreated, can progress to severe arthritis, cardiac problems, neurologic complications, ocular problems, gastrointestinal complaints, and hepatitis.
Diagnosis is made by blood work (Lyme titer via ELISA and Western Blot). If there are neurologic symptoms, the CSF needs to be tested for meningitis.
Treatment includes:
1. Tick removal
2. Contact your primary physician
3. Antibiotics (Doxycycline, Amoxicillin, or Cefuroxime) for at least 21 days
4. If the symptoms are severe, IV antibiotics may be necessary
Prevention includes:
1. Wear enclosed shoes and light-colored clothing to spot ticks
2. Check clothes and any exposed skin frequently for ticks while outdoors
3. Stay on cleared, well-traveled trails
4. Use insect repellant containing DEET (Diethyl-meta-toluamide) on skin or clothes
5. Avoid sitting directly on the ground or on stone walls
6. Keep long hair tied back
7. Do a full-body tick-check at the end of the day (also check children and pets)
To remove a tick, follow these steps:
1. Using a pair of pointed tweezers, grasp the tick by the head right where it enters the skin. Do not grasp the tick by the body.
2. Pull firmly and steadily directly outward. Dn not twist the tick out or apply petroleum jelly, a hot match, alcohol or any other irritant to the tick in an attempt to get it to back out.
3. Place the tick in a vial of alcohol to kill it.
4. Clean the bite wound
Contact your primary physician for more information.
Also check the CDC link on Lyme Disease.
Have a safe Thanksgiving Holiday!
Wednesday, November 18, 2009
Honey and Babies
During my newborn intake exams, I usually give a fair amount of education and advice. The one advice that I get the most perplexed looks is the recommendation of NO honey for babies.
Honey should not be given to infants one year or younger.
The reason is an infection called botulism. The botulinum spore is found in honey. When a baby ingests honey, the spores grow in the digestive tract and then the toxin spreads into the body. The infection does not typically cause problems in adults or children but in babies can cause a multitude of complications.
Most cases of infant botulism are mild but few are progressive.
The potential signs and symptoms include:
1. Constipation (typically first sign) in two to thirty days following ingestion
2. Increased listlessness/lethargy
3. Poor cry
4. Decreased feeding
5. Diminished gag or suck (as the disease progresses)
6. Loss of head control
7. Respiratory arrest
8. Temporary paralysis
If the signs and symptoms are progressing, contact your primary physician. Diagnosis can be made with lab work. Some babies may need to be hospitalized.
Treatment is supportive care. Some infants may need mechanical ventilation as they recover. There is an anti-toxin available to help with treatment.
The fatality rate is less than 1% due to increased awareness and prevention.
Honey should never be placed on the pacifier to sweeten it or added to baby food.
The bottomline is do not give honey (of any kind) to infants one year of age or younger.
Contact your primary physician for more information. Thank you.
Honey should not be given to infants one year or younger.
The reason is an infection called botulism. The botulinum spore is found in honey. When a baby ingests honey, the spores grow in the digestive tract and then the toxin spreads into the body. The infection does not typically cause problems in adults or children but in babies can cause a multitude of complications.
Most cases of infant botulism are mild but few are progressive.
The potential signs and symptoms include:
1. Constipation (typically first sign) in two to thirty days following ingestion
2. Increased listlessness/lethargy
3. Poor cry
4. Decreased feeding
5. Diminished gag or suck (as the disease progresses)
6. Loss of head control
7. Respiratory arrest
8. Temporary paralysis
If the signs and symptoms are progressing, contact your primary physician. Diagnosis can be made with lab work. Some babies may need to be hospitalized.
Treatment is supportive care. Some infants may need mechanical ventilation as they recover. There is an anti-toxin available to help with treatment.
The fatality rate is less than 1% due to increased awareness and prevention.
Honey should never be placed on the pacifier to sweeten it or added to baby food.
The bottomline is do not give honey (of any kind) to infants one year of age or younger.
Contact your primary physician for more information. Thank you.
Tuesday, November 17, 2009
Quotations
"The only way to keep your health is to eat what you don't want, drink what you don't like, and do what you'd rather not."
Mark Twain
"He who has health has hope, and he who has hope has everything."
Arabian Proverb
"Nature, time and patience are three great physicians."
H.G. Bohn
Mark Twain
"He who has health has hope, and he who has hope has everything."
Arabian Proverb
"Nature, time and patience are three great physicians."
H.G. Bohn
Update
Several patients made a suggestion that I should be more regular on my blog postings. Therefore, I will post a new case every Monday. Also, check out some of my older posts. I hope this blog has been informative. Thank you.
Monday, November 16, 2009
H1N1 Questions and Answers
I was recently on WBOC news to answer questions about the H1N1 influenza. WBOC arranged a telephone and online chat helpline which was very successful and helped alleviate some of the concerns about the flu. Here are some of the more frequently asked questions:
Who qualifies for the vaccine?
1. Pregnant women
2. People who live with or care for children younger than 6 months of age
3. Healthcare and emergency medical services personnel
4. Persons between the ages of 6 months and 24 years old
5. People ages of 25 through 64 years of age with chronic health disorders or compromised immune systems.
What are some of the chronic health disorders?
1. Cerebral palsy, epilepsy (seizure disorders), stroke, intellectual disability (mental retardation), moderate to severe developmental delay, muscular dystrophy, or spinal cord injury
2. Chronic lung disease, asthma, chronic obstructive pulmonary disease, cystic fibrosis
3. Congenital heart disease, congestive heart failure, coronary artery disease, heart attack
4. Sickle cell disease
5. Diabetes
6. Kidney disorders, end stage renal disease
7. Liver disorders, cirrhosis, hepatitis, Crohns disease
8. Metabolic disorders and mitochondrial disorders
9. Weakened immune system due to disease or medication (such as people with HIV, cancer, or those on chronic steroids)
10. People younger than 19 years of age who are receiving long-term aspirin therapy
This list is NOT a complete list, please contact your physician for further information
Why are individuals over 65 years of age not being vaccinated?
Current studies indicate the risk for infection among persons age 65 or older is less than the risk for younger age groups. Therefore, as vaccine supply and demand for vaccine among younger age groups is being met, providers should eventually offer vaccination to people over the age of 65.
Is the H1N1 vaccine safe?
Yes. The H1N1 vaccine is FDA approved. The vaccine is made just like the seasonal flu.
Who should NOT get the vaccine?
1. People who have a severe allergy to chicken eggs
2. People who have had a severe reaction to an influenza vaccination
3. People who developed Guillain-Barré syndrome (GBS) within 6 weeks of getting an influenza vaccine previously
4. Children younger than 6 months of age (influenza vaccine is not approved for this age group),
5. People who have a moderate-to-severe illness with a fever (they should wait until they recover to get vaccinated.)
What are the side effects of the vaccine?
1. Soreness, redness, or swelling where the shot was given
2. Fainting (mainly adolescents)
3. Headache
4. Muscle aches
5. Mild fever
6. Nausea.
If these problems occur, they usually begin soon after the shot and last 1-2 days.
I received my vaccine. What are the concerning side effects?
After vaccination you should look for any unusual signs or symptoms, such as a high fever or behavior changes. Signs of a serious allergic reaction can include difficulty breathing, hoarseness or wheezing, swelling around the eyes or lips, hives, paleness, weakness, a fast heart beat or dizziness. If any unusual condition occurs following vaccination, seek medical attention right immediately!!!
What is the difference between the seasonal flu and the H1N1 flu?
The symptoms of both are very similar, which includes fever, cough, sore throat, runny or stuffy nose, body aches, headache, chills, fatigue, vomiting and diarrhea.
The main difference is H1N1 is a novel virus which means it is a new strand to humans. Children and young adults are prone to getting this strand because their immune system has no previous experience battling it. Older adults may have some immunity protection from prior exposures to similar viral strands.
My child has asthma. Can he get the nasal mist vaccine?
No. The mist is only for healthy individuals 2 years to 49 years of age who are not pregnant.
I am breastfeeding. Can I get the vaccine?
Yes.
My child has asthma. The school is giving out the mist form. Can he go to school?
Yes. It is safe for a child with asthma to go to school and be around the children who received the mist vaccine. He/she should not get the mist vaccine but instead receive the injectable form.
The estimated risk of getting infected with vaccine virus after close contact with a person vaccinated with the nasal-spray flu vaccine is low (0.6%-2.4%).
What is the difference between the nasal mist and the injectable vaccine?
The nasal mist is made with a weakened, live virus. The injectable is made with an inactivated killed virus.
When does immunity begin?
8 days to two weeks
Why does my 5 year old need two shots?
The CDC recommends that the two doses of 2009 H1N1 vaccine be separated by 4 weeks in children 9 years of age and younger. The first dose only provides moderate immunity. The second dose provides up to 96% effectivity.
Where do I get the vaccine?
If you fall in the priority groups, contact your primary physician. If it is unavailable, contact the state health department. WBOC has the links on their webpage.
How many people have died from the H1N1 flu?
There have been approximately 4,000 deaths.
Are more vaccines coming?
Yes. The Federal Government has purchased about 250 million vaccines and about 40 million have been already allocated.
I do not qualify for the vaccine. How do I prevent myself from catching the flu?
1. Cover your nose and mouth with a tissue or elbow/upper arm when you cough or sneeze.
2. Wash your hands often with soap and water. If soap and water are not available, use an alcohol-based hand rub.
3. Avoid touching your eyes, nose or mouth.
4. Try to avoid close contact with sick people.
I think I have the flu. How do I get tested?
Testing is done via nasal swab/washing. Testing is performed by the physician's discretion but is currently limited to hospitalized individuals and severely ill patients.
Do I need the H1N1 vaccine if I had the H1N1 flu?
If the flu was confirmed to be H1N1, it is not necessary to be vaccinated.
Contact your primary physician for more information. Other useful websites include
CDC
WBOC flu resource page
Thank you.
Wednesday, November 11, 2009
Aspirin and Children
Due to the increased number of pediatric flu and cold cases, the use of Tylenol and ibuprofen has elevated. Recently, a patient asked me why not a baby aspirin.
Aspirin should not be given to children because it may cause a rare and potentially fatal disease called Reye's Syndrome.
Reye's syndrome is a condition which causes encephalopathy (disease of the brain) with brain swelling and fatty infiltration of the liver. The mechanism is unknown but it has been associated with aspirin usage during a viral illness. Reye's syndrome is rare...about 2 reported cases per year and mortality has decreased due to early and aggressive intervention. The best way to prevent this disease is to not give children aspirin. Usually, the first signs of this syndrome are severe vomiting and lethargy several days after the viral illness, so contact your physician immediately.
Other products (not a complete list) containing aspirin (or salicylates...aspirin is a type of salicylate drug) include:
1. Alka Seltzer
2. Pepto-Bismol
3. Bufferin
4. Excedrin
5. Pamprin
6. Ecotrin
Aspirin may be given to children with certain medical conditions (but only with physician supervision) including Kawasaki's Disease, heart disease, rheumatoid arthritis, blood clot prevention in children with blood disorders, or rheumatic fever.
Therefore, if your child has a fever, try the following treatments:
1. Lots of fluids
2. Acetaminophen (Tylenol)
3. Ibuprofen (Motrin/Advil)
4. Lukewarm bath
5. Light cotton pajamas
6. Keeping the room temperature between 70-74 degrees
Bottom line- No aspirin for children
For more information, talk to your primary physician. Thank you.
Aspirin should not be given to children because it may cause a rare and potentially fatal disease called Reye's Syndrome.
Reye's syndrome is a condition which causes encephalopathy (disease of the brain) with brain swelling and fatty infiltration of the liver. The mechanism is unknown but it has been associated with aspirin usage during a viral illness. Reye's syndrome is rare...about 2 reported cases per year and mortality has decreased due to early and aggressive intervention. The best way to prevent this disease is to not give children aspirin. Usually, the first signs of this syndrome are severe vomiting and lethargy several days after the viral illness, so contact your physician immediately.
Other products (not a complete list) containing aspirin (or salicylates...aspirin is a type of salicylate drug) include:
1. Alka Seltzer
2. Pepto-Bismol
3. Bufferin
4. Excedrin
5. Pamprin
6. Ecotrin
Aspirin may be given to children with certain medical conditions (but only with physician supervision) including Kawasaki's Disease, heart disease, rheumatoid arthritis, blood clot prevention in children with blood disorders, or rheumatic fever.
Therefore, if your child has a fever, try the following treatments:
1. Lots of fluids
2. Acetaminophen (Tylenol)
3. Ibuprofen (Motrin/Advil)
4. Lukewarm bath
5. Light cotton pajamas
6. Keeping the room temperature between 70-74 degrees
Bottom line- No aspirin for children
For more information, talk to your primary physician. Thank you.
Monday, November 9, 2009
Cholesterol and Diet
Over 100 million Americans have elevated cholesterol (over 200 mg/dL)!!!
That is a staggering statistic. Like most primary physicians, we see quite a few patients with high cholesterol. We try various treatments to help bring the numbers down including diet, exercise, and medications. Medications definitely help but I am a fan of at least attempting diet modification.
Cholesterol is a fat-like substance that the body needs to function. It is used to produce hormones, healthy cells, fat-soluble vitamins, and bile acids to break down fat. Unfortunately, when the levels exceeds the body's needs, the excess deposits on the arterial walls and creates blockages. These blockages lead to heart attacks and strokes. Cholesterol is basically broken down to good and bad cholesterol.
Good cholesterol (high density lipoprotein or HDL) transports bad cholesterol from the tissues of the body to the liver so it can be eliminated. You want this level as High as possible.
Bad cholesterol (low density lipoprotein or LDL) at high levels build up on the walls of the arteries and lead to blockages. You want this level as Low as possible.
Triglycerides are a type of fat in the body and blood stream and also contribute to blockages.
The numerical goals are:
Total Cholesterol under 200 mg/dL
LDL under 100 mg/dL
HDL preferably over 50 mg/dL
Triglyceride under 150 mg/dL
Recently, I have been recommending these foods (in conjunction with exercise) to help improve cholesterol levels without the use of medications.
Lowers LDL
Red grapefruit: 1 daily reduces levels by 20 percent
Steel-cut oatmeal: 3/4 cup daily reduces levels by 15 percent
Pecans: 1 oz daily reduces levels by 13 percent
Pistachios: 3 oz daily reduces levels by 12 percent
Promise activ spread: 3 servings daily reduces levels by 10 percent
Macadamia nuts: 1.5 oz daily reduces levels by 9 percent
Pinto beans: 1/2 cup daily reduces levels by 7 percent
Walnuts and almonds 1 oz daily reduces levels by 7 percent
Peanuts: 1 oz daily reduces levels by 6 percent
Raises HDL
Orange juice: Three 8 oz glasses daily boosts levels by 21 percent
Hazelnuts: 1.5 oz daily boosts levels by 13 percent
Dark chocolate: 2.5 oz daily boosts levels by 11 percent
Extra-virgin olive oil: 2 Tbsp daily boosts levels by 4 percent
Lowers triglycerides
Fish oil: 4 grams daily reduces levels up to 45 percent
Peanuts: 3 oz daily reduces levels by up to 24 percent
Pistachios: 2 to 3 oz daily reduces levels by 10 points
The American Heart Association also has a good patient handout about lowering cholesterol.
Click here
Medications may be necessary, especially when there are multiple risk factors for heart disease and/or stroke. Talk to your physician about a treatment plan (including diet and exercise) to help lower cholesterol. Hopefully with improved health, we can lower the amount of heart disease in this country.
That is a staggering statistic. Like most primary physicians, we see quite a few patients with high cholesterol. We try various treatments to help bring the numbers down including diet, exercise, and medications. Medications definitely help but I am a fan of at least attempting diet modification.
Cholesterol is a fat-like substance that the body needs to function. It is used to produce hormones, healthy cells, fat-soluble vitamins, and bile acids to break down fat. Unfortunately, when the levels exceeds the body's needs, the excess deposits on the arterial walls and creates blockages. These blockages lead to heart attacks and strokes. Cholesterol is basically broken down to good and bad cholesterol.
Good cholesterol (high density lipoprotein or HDL) transports bad cholesterol from the tissues of the body to the liver so it can be eliminated. You want this level as High as possible.
Bad cholesterol (low density lipoprotein or LDL) at high levels build up on the walls of the arteries and lead to blockages. You want this level as Low as possible.
Triglycerides are a type of fat in the body and blood stream and also contribute to blockages.
The numerical goals are:
Total Cholesterol under 200 mg/dL
LDL under 100 mg/dL
HDL preferably over 50 mg/dL
Triglyceride under 150 mg/dL
Recently, I have been recommending these foods (in conjunction with exercise) to help improve cholesterol levels without the use of medications.
Lowers LDL
Red grapefruit: 1 daily reduces levels by 20 percent
Steel-cut oatmeal: 3/4 cup daily reduces levels by 15 percent
Pecans: 1 oz daily reduces levels by 13 percent
Pistachios: 3 oz daily reduces levels by 12 percent
Promise activ spread: 3 servings daily reduces levels by 10 percent
Macadamia nuts: 1.5 oz daily reduces levels by 9 percent
Pinto beans: 1/2 cup daily reduces levels by 7 percent
Walnuts and almonds 1 oz daily reduces levels by 7 percent
Peanuts: 1 oz daily reduces levels by 6 percent
Raises HDL
Orange juice: Three 8 oz glasses daily boosts levels by 21 percent
Hazelnuts: 1.5 oz daily boosts levels by 13 percent
Dark chocolate: 2.5 oz daily boosts levels by 11 percent
Extra-virgin olive oil: 2 Tbsp daily boosts levels by 4 percent
Lowers triglycerides
Fish oil: 4 grams daily reduces levels up to 45 percent
Peanuts: 3 oz daily reduces levels by up to 24 percent
Pistachios: 2 to 3 oz daily reduces levels by 10 points
The American Heart Association also has a good patient handout about lowering cholesterol.
Click here
Medications may be necessary, especially when there are multiple risk factors for heart disease and/or stroke. Talk to your physician about a treatment plan (including diet and exercise) to help lower cholesterol. Hopefully with improved health, we can lower the amount of heart disease in this country.
Sunday, November 8, 2009
The Power of Yogurt
Whenever I prescribe antibiotics, I usually recommend eating yogurt. I have also recommended yogurt to patients with lactose intolerance and irritable bowel syndrome. The reason is Probiotics.
Probiotics are microorganisms (bacteria and a few yeast types) that are similar to the beneficial organisms in our digestive system (the gut has about 400 types of probiotic organisms). They are also called "good bacteria." They promote a healthy digestive tract and reduces the number of harmful bacteria. The most common probiotics are Lactobacillus and Bifidobacterium. Probiotics are found in yogurt, fermented and unfermented milk, miso, soy drinks, fermented foods (pickled vegetables, kimchi, sauerkraut, etc...), and dietary supplements.
The GI tract needs to maintain a healthy balance of good bacteria. When antibiotics are taken, the good bacteria may also be killed, changing the balance and leading to gas, cramping, or diarrhea (and potentially Clostridium difficile colitis). Studies have shown there is up to a 50% reduction in antibiotic associated diarrhea with the use of probiotics.
Other potential benefits by taking probiotics include:
1. Managing lactose intolerance
2. Suppress or reduce bad organisms associated with traveler's diarrhea, infectious diarrhea, irritable bowel syndrome, vaginal infections, Helicobacter pylori gastritis, inflammatory bowel disease, and tooth decay
3. Prevent colon cancer...studies pending
4. Possibly reducing blood pressure and cholesterol
5. Improving immune function
6. Managing eczema
7. Improving irritable bowel syndrome symptoms
8. Reducing inflammation associated with colitis
Probiotics are considered safe. Dietary supplements (capsules, powder, liquid extracts) are not regulated by the FDA so consult your primary physician for more information.
Yogurt is a good source of probiotics. Make sure the label states "active culture." Probiotics can potentially help with overall health. Studies are ongoing.
When taking antibiotics though, consider consuming two servings of yogurt a day to reduce antibiotic associated complications like diarrhea, gas, cramping, and nausea.
As always, talk to your health care professional before you start any supplements.
Probiotics are microorganisms (bacteria and a few yeast types) that are similar to the beneficial organisms in our digestive system (the gut has about 400 types of probiotic organisms). They are also called "good bacteria." They promote a healthy digestive tract and reduces the number of harmful bacteria. The most common probiotics are Lactobacillus and Bifidobacterium. Probiotics are found in yogurt, fermented and unfermented milk, miso, soy drinks, fermented foods (pickled vegetables, kimchi, sauerkraut, etc...), and dietary supplements.
The GI tract needs to maintain a healthy balance of good bacteria. When antibiotics are taken, the good bacteria may also be killed, changing the balance and leading to gas, cramping, or diarrhea (and potentially Clostridium difficile colitis). Studies have shown there is up to a 50% reduction in antibiotic associated diarrhea with the use of probiotics.
Other potential benefits by taking probiotics include:
1. Managing lactose intolerance
2. Suppress or reduce bad organisms associated with traveler's diarrhea, infectious diarrhea, irritable bowel syndrome, vaginal infections, Helicobacter pylori gastritis, inflammatory bowel disease, and tooth decay
3. Prevent colon cancer...studies pending
4. Possibly reducing blood pressure and cholesterol
5. Improving immune function
6. Managing eczema
7. Improving irritable bowel syndrome symptoms
8. Reducing inflammation associated with colitis
Probiotics are considered safe. Dietary supplements (capsules, powder, liquid extracts) are not regulated by the FDA so consult your primary physician for more information.
Yogurt is a good source of probiotics. Make sure the label states "active culture." Probiotics can potentially help with overall health. Studies are ongoing.
When taking antibiotics though, consider consuming two servings of yogurt a day to reduce antibiotic associated complications like diarrhea, gas, cramping, and nausea.
As always, talk to your health care professional before you start any supplements.
Thursday, November 5, 2009
Quotation
"Drugs are not always necessary. Belief in recovery always is."
Norman Cousins
"The doctor of the future will give no medicine but will interest his patients in the care of the human frame, in diet and in the cause and prevention of disease."
Thomas Edison
Norman Cousins
"The doctor of the future will give no medicine but will interest his patients in the care of the human frame, in diet and in the cause and prevention of disease."
Thomas Edison
Wednesday, November 4, 2009
Shoulder pain
During baseball season, I saw a 17 year old male come to the office for right shoulder pain. He was playing summer ball as a pitcher and centerfielder. On one of the games, a ball was hit into the gap and he attempted to make a diving catch. Unfortunately, he did not make the catch and started writhing in pain. He was sent to the emergency room for evaluation. He explained how he could not move his arm and had to keep it braced. According to records, he had several xrays and underwent a shoulder reduction. He was told to follow-up in the office and obtain an orthopedic evaluation.
The patient was diagnosed with a shoulder dislocation and after months of treatment (including rest and then therapy), he was throwing again.
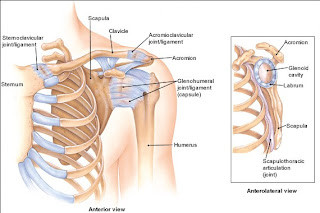
Shoulder dislocation (or glenohumeral dislocation) occurs when the head of the upper arm bone (humerus) is out of the socket of the scapula (glenoid). Typically, it is caused by direct trauma or sports injury (younger patients) or falls (older patients). In this patient, it was caused by a fall on an outstretched arm and also indirectly being a pitcher (possibly causing instability). About 90% of the time, the dislocation is anterior, where the head of the humerus is sitting in front of the shoulder blade. Posterior dislocations are rare and are seen after electrocutions or seizures.
The patient was diagnosed with a shoulder dislocation and after months of treatment (including rest and then therapy), he was throwing again.

Shoulder dislocation (or glenohumeral dislocation) occurs when the head of the upper arm bone (humerus) is out of the socket of the scapula (glenoid). Typically, it is caused by direct trauma or sports injury (younger patients) or falls (older patients). In this patient, it was caused by a fall on an outstretched arm and also indirectly being a pitcher (possibly causing instability). About 90% of the time, the dislocation is anterior, where the head of the humerus is sitting in front of the shoulder blade. Posterior dislocations are rare and are seen after electrocutions or seizures.
The signs and symptoms of a dislocation include:
1. PAIN
2. Difficulty moving the arm
3. Cavity in the shoulder area
4. Arm locked in place
Diagnosis is made by examination, history, and radiographs.
Treatment includes:
1. Reduction or "popping" the shoulder back into place.
2. Immobilization for one to three weeks
3. Rehabilitation, improving range of motion and strengthening
4. Possible surgical intervention
Depending on the sport and severity, athletes can return to play 3-4 months after injury.
Here are some statistics regarding shoulder dislocations:
1. About 90% who experience a SD under 20 years of age will experience a second SD.
2. Patients (30 years or younger) who experience a SD have a 50% recurrence rate.
3. The shoulder is the most commonly dislocated joint in the body.
4. 95% of SDs occur due to a traumatic event.
Shoulder pain can be caused by other problems including rotator cuff injury, clavicular fractures, shoulder separation (injury of the acromioclavicular joint), humeral fractures, and non-orthopedic conditions such as pneumonia, heart disease, and peptic ulcer disease. The history and physical are the keys to determining the etiology of shoulder pain.
Contact your physician for more information. Thank you and have a nice day.
Monday, November 2, 2009
Soft Drinks
My wife recently went to a seminar on the bad effects of soft drinks. Ever since then, I was banned from drinking my usual Diet Coke. It has been difficult...it was my daily caffeine fix, but the sacrifice was warranted.
The consumption of soft drinks has increased by 500% over the past fifty years. Americans drink about 50 gallons of soft drinks per person per year. Therefore, the soda industry grosses $40-50 billion per year.
Why are soft drinks bad?
Soft drinks contain simple sugars or artificial sweeteners, caffeine, and food additives. Due to their ingredients, soft drinks have been linked to many health problems.
12 ounces of regular soda contains about 10 teaspoons of sugar!!! A can of regular soda has about 150 calories (empty calories). Think about what this could cause...weight gain, diabetes, depressed immune system, and heart disease. Diet soda has also been implicated in weight gain so beware!!!
Sodas (regular and diet) increase the risk for tooth decay. The acid dissolves the enamel in twenty minutes. The more you drink, the worse the decay. The acid has been linked to calcium loss which contributes to the development of osteoporosis and also reflux disease (heartburn).
Of note, the pH of soda is about 2-4, while human blood pH is about 7.35.
Caffeine is linked to anxiety and sleep disorders. It can also increase blood pressure, cause palpitations and possibly reduce calcium stores.
Soft drinks also contain sodium which can contribute to elevated blood pressure and dehydration.
Soft drinks typically have no nutritional value. Unfortunately, many children are replacing milk, water, and fruit drinks with sodas. Also beware of energy drinks...they contain larger doses of sugar and caffeine plus other stimulants.
Interestingly, soft drinks can remove rust off metal surfaces, clean corrosion from car batteries, and possible clear clogged drains.
Due to my wife's advice, I have been drinking more water and fruit juices. Try to replace the sodas with water, teas (loaded with antioxidants), milk, and fruit juices (low sugar of course).
Hope this was informative.
The consumption of soft drinks has increased by 500% over the past fifty years. Americans drink about 50 gallons of soft drinks per person per year. Therefore, the soda industry grosses $40-50 billion per year.
Why are soft drinks bad?
Soft drinks contain simple sugars or artificial sweeteners, caffeine, and food additives. Due to their ingredients, soft drinks have been linked to many health problems.
12 ounces of regular soda contains about 10 teaspoons of sugar!!! A can of regular soda has about 150 calories (empty calories). Think about what this could cause...weight gain, diabetes, depressed immune system, and heart disease. Diet soda has also been implicated in weight gain so beware!!!
Sodas (regular and diet) increase the risk for tooth decay. The acid dissolves the enamel in twenty minutes. The more you drink, the worse the decay. The acid has been linked to calcium loss which contributes to the development of osteoporosis and also reflux disease (heartburn).
Of note, the pH of soda is about 2-4, while human blood pH is about 7.35.
Caffeine is linked to anxiety and sleep disorders. It can also increase blood pressure, cause palpitations and possibly reduce calcium stores.
Soft drinks also contain sodium which can contribute to elevated blood pressure and dehydration.
Soft drinks typically have no nutritional value. Unfortunately, many children are replacing milk, water, and fruit drinks with sodas. Also beware of energy drinks...they contain larger doses of sugar and caffeine plus other stimulants.
Interestingly, soft drinks can remove rust off metal surfaces, clean corrosion from car batteries, and possible clear clogged drains.
Due to my wife's advice, I have been drinking more water and fruit juices. Try to replace the sodas with water, teas (loaded with antioxidants), milk, and fruit juices (low sugar of course).
Hope this was informative.
Sunday, November 1, 2009
Vitamin D Deficiency
Vitamin D Deficiency is becoming a more prevalent health issue. Here are some surprising statistics that confirm this growing problem:
1. Approximately 9% of children are Vitamin D deficient
2. About 60% of children are insufficient (the level prior to being deficient)
3. 40% of Americans are deficient
4. About 30% of physicians and medical students are Vitamin D deficient!!!
5. 48% of young girls are deficient
Why is Vitamin D important?
Deficiency may cause osteoporosis, Rickets (childhood disorder causing growth impairment and deformity of the long bones), fatigue, bone pain, increased risk of falls, muscle aches, low back pain, and osteomalacia (bone thinning disorder).
It may also play a role in the following conditions:
1. Cardiovascular Heart Disease
2. Colon Cancer
3. Depression
4. Diabetes
5. Multiple Sclerosis
6. Hypertension
7. Asthma in children
What are the causes/risk factors of Vitamin D deficiency?
1. Inadequate sunlight exposure (UVB rays)
2. Inadequate consumption/diet
3. Dark skin
4. Certain digestive tract disorders
5. Obesity
6. Sedentary lifestyle
7. Breastfeeding exclusively with no Vitamin D supplementation
8. Age greater than 65
9. Medications interfering with absorption or metabolism (steroids, seizure medications)
10. Liver disease
11. Kidney Disease
Diagnosis is made by blood work. Deficiency is defined as a serum 25-hydroxyvitamin D level of less than 20 ng per mL (50 nmol per L), and insufficiency is defined as a serum 25-hydroxyvitamin D level of 20 to 30 ng per mL (50 to 75 nmol per L).
Treatment and sources of Vitamin D
1. Sunlight. People obtain 90% of Vitamin D from the sunshine. Researchers have suggested 5-30 minutes of sun exposure at least twice a week to maintain adequate status.
2. Food. Cod liver oil, mushrooms, salmon, mackerel, sardines, tuna, fortified orange juice, fortified milk and milk products, eggs, and fortified cereals.
3. Vitamin D supplements with pills or injection.
The recommended adequate intake dose for Vitamin D is:
1. Children and adolescents: 200 IU daily
2. Adults up to 50 years: 200 IU daily
3. Adults 51-70: 400 IU daily
4. Adults 71 and over: 600 IU daily
The Pediatric Academy recently recommended doubling the intake for children to 400 IU daily.
In adults, Vitamin D deficiency should be promptly treated with the above sources and then the maintenance dosages should be between 800-1000 IU daily.
Be aware of Vitamin D toxicity. Signs and symptoms include headache, nausea, metallic taste, and pancreatitis.
Please contact your primary physician for more information on Vitamin D. Thank you and have a nice day.
1. Approximately 9% of children are Vitamin D deficient
2. About 60% of children are insufficient (the level prior to being deficient)
3. 40% of Americans are deficient
4. About 30% of physicians and medical students are Vitamin D deficient!!!
5. 48% of young girls are deficient
Why is Vitamin D important?
Deficiency may cause osteoporosis, Rickets (childhood disorder causing growth impairment and deformity of the long bones), fatigue, bone pain, increased risk of falls, muscle aches, low back pain, and osteomalacia (bone thinning disorder).
It may also play a role in the following conditions:
1. Cardiovascular Heart Disease
2. Colon Cancer
3. Depression
4. Diabetes
5. Multiple Sclerosis
6. Hypertension
7. Asthma in children
What are the causes/risk factors of Vitamin D deficiency?
1. Inadequate sunlight exposure (UVB rays)
2. Inadequate consumption/diet
3. Dark skin
4. Certain digestive tract disorders
5. Obesity
6. Sedentary lifestyle
7. Breastfeeding exclusively with no Vitamin D supplementation
8. Age greater than 65
9. Medications interfering with absorption or metabolism (steroids, seizure medications)
10. Liver disease
11. Kidney Disease
Diagnosis is made by blood work. Deficiency is defined as a serum 25-hydroxyvitamin D level of less than 20 ng per mL (50 nmol per L), and insufficiency is defined as a serum 25-hydroxyvitamin D level of 20 to 30 ng per mL (50 to 75 nmol per L).
Treatment and sources of Vitamin D
1. Sunlight. People obtain 90% of Vitamin D from the sunshine. Researchers have suggested 5-30 minutes of sun exposure at least twice a week to maintain adequate status.
2. Food. Cod liver oil, mushrooms, salmon, mackerel, sardines, tuna, fortified orange juice, fortified milk and milk products, eggs, and fortified cereals.
3. Vitamin D supplements with pills or injection.
The recommended adequate intake dose for Vitamin D is:
1. Children and adolescents: 200 IU daily
2. Adults up to 50 years: 200 IU daily
3. Adults 51-70: 400 IU daily
4. Adults 71 and over: 600 IU daily
The Pediatric Academy recently recommended doubling the intake for children to 400 IU daily.
In adults, Vitamin D deficiency should be promptly treated with the above sources and then the maintenance dosages should be between 800-1000 IU daily.
Be aware of Vitamin D toxicity. Signs and symptoms include headache, nausea, metallic taste, and pancreatitis.
Please contact your primary physician for more information on Vitamin D. Thank you and have a nice day.
Subscribe to:
Posts (Atom)